Definition:
|
The IDEA 2004 (Individuals with Disabilities Education Act) definition of Autistic Spectrum Disorder is "a developmental disability significantly affecting verbal and nonverbal communication and social interaction, generally evident before age three, that adversely affects a child's educational performance. Other characteristics often associated with autism are engaging in repetitive activities and stereotyped movements, resistance to environmental change or change in daily routines, and unusual responses to sensory experiences. The termis autism does not apply if the child’s educational performance is adversely affected primarily because the child has an emotional disturbance" (IDEA-Building the Legacy of IDEA 2004, 2006).
The definition of ASD according the the State of Minnesota is: "Autism spectrum disorders (ASD)" means a range of pervasive developmental disorders, with onset in childhood, that adversely affect a pupil's functioning and result in the need for special education instruction and related services. ASD is a disability category characterized by an uneven developmental profile and a pattern of qualitative impairments in several areas of development, including social interaction, communication, or the presence of restricted, repetitive, and stereotyped patterns of behavior, interests, and activities. These core features may present themselves in a wide variety of combinations that range from mild to severe, and the number of behavioral indicators present may vary. ASD may include Autistic Disorder, Childhood Autism, Atypical Autism, Pervasive Developmental Disorder Not Otherwise Specified, Asperger's Disorder, or other related pervasive developmental disorders" (Minnesota Administrative Rules, 2007). |
|
Eligibility:
Under the Minnesota State Law the students are eligible to qualify for ASD services if:
"A multidisciplinary team shall determine that pupil is eligible and in need of special education instruction and related services if the pupil meets the criteria in items A and B. A determination of eligibility must be supported by information collected from multiple settings and sources.
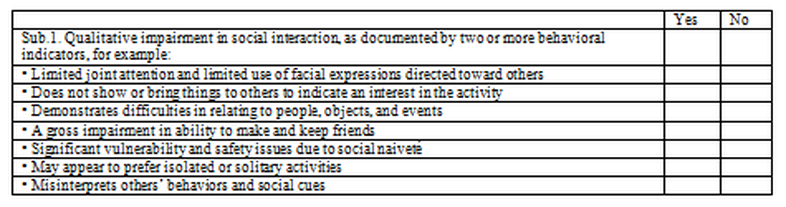
A. An educational evaluation must address all three core features in subitems (1) to (3). The team must document that the pupil demonstrates patterns of behavior described in at least two of these subitems, one of which must be subitem (1).
The behavioral indicators demonstrated must be atypical for the pupil's developmental level. The team shall document behavioral indicators through at least two of these methods: structured interviews with parents, autism checklists, communication and developmental rating scales, functional behavior assessments, application of diagnostic criteria from the current Diagnostic and Statistical Manual (DSM), informal and standardized evaluation instruments, or intellectual testing.
(1) Qualitative impairment in social interaction, as documented by two or more behavioral indicators, for example: limited joint attention and limited use of facial expressions directed toward others; does not show or bring things to others to indicate an interest in the activity; demonstrates difficulties in relating to people, objects, and events; a gross impairment in ability to make and keep friends; significant vulnerability and safety issues due to social naivete; may appear to prefer isolated or solitary activities; misinterprets others' behaviors and social cues.
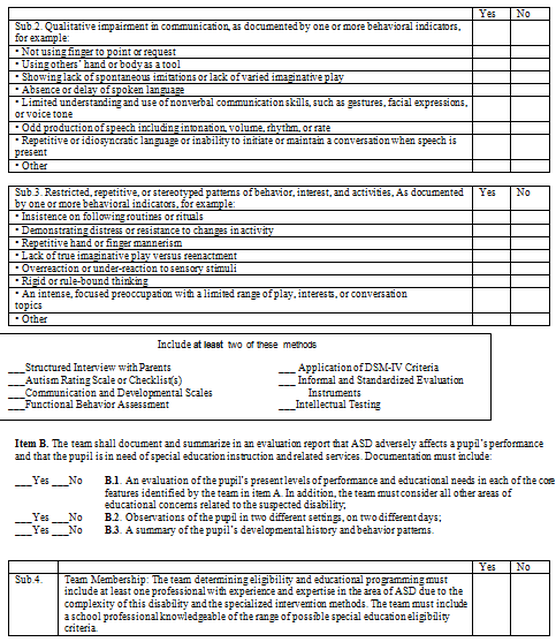
(2) Qualitative impairment in communication, as documented by one or more behavioral indicators, for example: not using finger to point or request; using others' hand or body as a tool; showing lack of spontaneous imitations or lack of varied imaginative play; absence or delay of spoken language; limited understanding and use of nonverbal communication skills such as gestures, facial expressions, or voice tone; odd production of speech including intonation, volume, rhythm, or rate; repetitive or idiosyncratic language or inability to initiate or maintain a conversation when speech is present.
(3) Restricted, repetitive, or stereotyped patterns of behavior, interest, and activities, as documented by one or more behavioral indicators, for example: insistence on following routines or rituals; demonstrating distress or resistance to changes in activity; repetitive hand or finger mannerism; lack of true imaginative play versus reenactment; overreaction or under-reaction to sensory stimuli; rigid or rule-bound thinking; an intense, focused preoccupation with a limited range of play, interests, or conversation topics.
B. The team shall document and summarize in an evaluation report that ASD adversely affects a pupil's performance and that the pupil is in need of special education instruction and related services. Documentation must include:
(1) an evaluation of the pupil's present levels of performance and educational needs in each of the core features identified by the team in item A. In addition, the team must consider all other areas of educational concern related to the suspected disability;
(2) observations of the pupil in two different settings, on two different days; and
(3) a summary of the pupil's developmental history and behavior patterns" (Minnesota Administrative Rules, 2007).
"A multidisciplinary team shall determine that pupil is eligible and in need of special education instruction and related services if the pupil meets the criteria in items A and B. A determination of eligibility must be supported by information collected from multiple settings and sources.
A. An educational evaluation must address all three core features in subitems (1) to (3). The team must document that the pupil demonstrates patterns of behavior described in at least two of these subitems, one of which must be subitem (1).
The behavioral indicators demonstrated must be atypical for the pupil's developmental level. The team shall document behavioral indicators through at least two of these methods: structured interviews with parents, autism checklists, communication and developmental rating scales, functional behavior assessments, application of diagnostic criteria from the current Diagnostic and Statistical Manual (DSM), informal and standardized evaluation instruments, or intellectual testing.
(1) Qualitative impairment in social interaction, as documented by two or more behavioral indicators, for example: limited joint attention and limited use of facial expressions directed toward others; does not show or bring things to others to indicate an interest in the activity; demonstrates difficulties in relating to people, objects, and events; a gross impairment in ability to make and keep friends; significant vulnerability and safety issues due to social naivete; may appear to prefer isolated or solitary activities; misinterprets others' behaviors and social cues.
(2) Qualitative impairment in communication, as documented by one or more behavioral indicators, for example: not using finger to point or request; using others' hand or body as a tool; showing lack of spontaneous imitations or lack of varied imaginative play; absence or delay of spoken language; limited understanding and use of nonverbal communication skills such as gestures, facial expressions, or voice tone; odd production of speech including intonation, volume, rhythm, or rate; repetitive or idiosyncratic language or inability to initiate or maintain a conversation when speech is present.
(3) Restricted, repetitive, or stereotyped patterns of behavior, interest, and activities, as documented by one or more behavioral indicators, for example: insistence on following routines or rituals; demonstrating distress or resistance to changes in activity; repetitive hand or finger mannerism; lack of true imaginative play versus reenactment; overreaction or under-reaction to sensory stimuli; rigid or rule-bound thinking; an intense, focused preoccupation with a limited range of play, interests, or conversation topics.
B. The team shall document and summarize in an evaluation report that ASD adversely affects a pupil's performance and that the pupil is in need of special education instruction and related services. Documentation must include:
(1) an evaluation of the pupil's present levels of performance and educational needs in each of the core features identified by the team in item A. In addition, the team must consider all other areas of educational concern related to the suspected disability;
(2) observations of the pupil in two different settings, on two different days; and
(3) a summary of the pupil's developmental history and behavior patterns" (Minnesota Administrative Rules, 2007).
Below you will find the ASD checklist used by the Saint Paul Public Schools to help determine if a student should be considered for eligibility (Autism Spectrum Disorder).
Statistical Information:
|
Currently, more than 3.5 million American have Autism Spectrum Disorder (Ostrow, 2014).
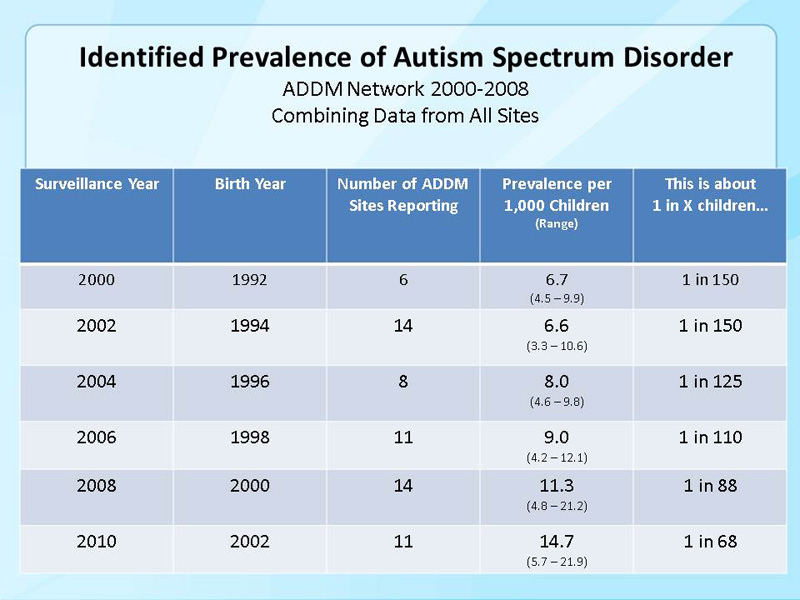
According to the CDC (2014), ASD is prevalent in 1 out of 68 births in the United States. In the United States, Autism is increasing drastically. In 2000, prevalence was approximately 1 in 150 and grew to 1 in 68 (Autism Spectrum Disorder (ASD): Data & Statistics, 2014). Approximately 1 out of 100 of the world population has a form of Autism Spectrum Disorder (Autism Spectrum Disorder (ASD): Data & Statistics, 2014). Each year, occurrences of ASD have increased 6-15% between the years 2002 and 2010 (Autism Spectrum Disorder (ASD): Data & Statistics, 2014). Annual autism costs, the majority of which are for adult services, are approximately $236-262 billion (Ostrow, 2014). Of all young adults (ages 19-23) with autism, 35% haven’t had a job or continued education after high school (Norton, 2012). The Minnesota Department of Education (2014) estimates the prevalence of ASD in Minnesota to be approximately 1 in 81. According to a recent study, Minneapolis school district has a prevalence of approximately 1 in 48 (Hewitt, 2013). 2014-2015 Mankato School District Statistics0-2 years old: 0 students
3-5 years old: 15 students 6-11 years old: 81 students 12-17 years old: 71 students 18-21 years old: 11 students Total: 178 students (Peterson, 2015) |
|
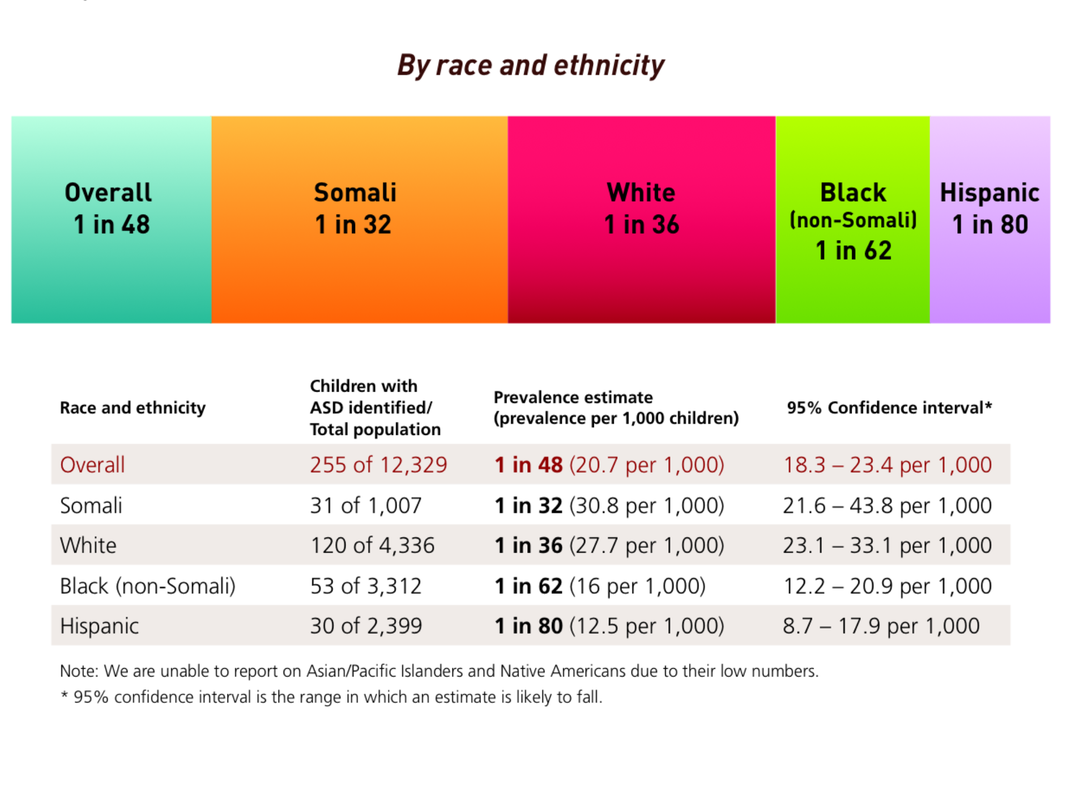
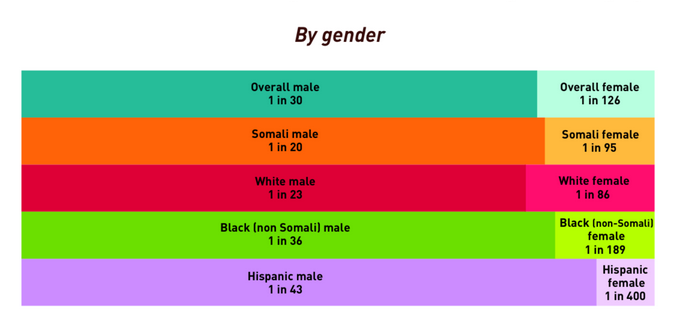
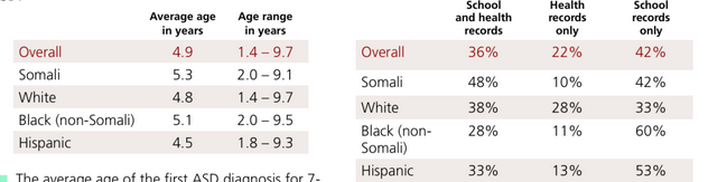
These charts show students that are identified as having ASD in the Minneapolis school district. The chart on the left shows the ages that the student was identified ASD and the chart on the right shows whether the student is identified ASD through school records, health records, or both.
The graphics above are retrieved from:
Hewitt, A., Gulaid, A., Hamre, K., Esler, A., Punyko, J., Reichle, J. & Reiff, M. (2013). Minneapolis Somali autism
spectrum disorder prevalence project: Community report 2013. Minneapolis, MN: University of Minnesota,
Institute on Community Integration, Research and Training Center on Community Living.
The graphics above are retrieved from:
Hewitt, A., Gulaid, A., Hamre, K., Esler, A., Punyko, J., Reichle, J. & Reiff, M. (2013). Minneapolis Somali autism
spectrum disorder prevalence project: Community report 2013. Minneapolis, MN: University of Minnesota,
Institute on Community Integration, Research and Training Center on Community Living.
By: Sarah Fischenish, Melanie Adam, and Nicole Zitur
